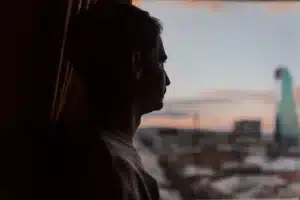
For millions of people, anxiety disorders—from generalized anxiety disorder (GAD) to panic disorder and social anxiety disorder—can be life-altering. But for some, even the best first-line treatments like cognitive behavioral therapy (CBT) and selective serotonin reuptake inhibitors (SSRIs) provide only partial relief. When symptoms persist despite appropriate care, clinicians refer to this as treatment-resistant anxiety (TRA)—a condition that demands new thinking, new tools, and a more personalized approach.
While standard therapies can transform lives, treatment-resistant anxiety reminds us that mental health isn’t one-size-fits-all. Some individuals continue to experience intense anxiety symptoms, panic attacks, or intrusive thoughts even after months of consistent care. For these patients, progress requires a deeper look—into biology, psychopharmacology, and lifestyle factors—so treatment can evolve beyond symptom management toward true, lasting recovery.
Understanding Treatment-Resistant Anxiety
In psychiatry, treatment-resistant anxiety disorders are typically defined by limited or no treatment response after at least two adequate trials of evidence-based interventions such as CBT or pharmacotherapy. According to the American Psychiatric Association (APA), treatment resistance can affect up to one-third of patients with GAD, panic disorder, or Obsessive-Compulsive Disorder (OCD).
Common predictors of resistance include:
- Comorbid psychiatric disorders like depressive disorder, bipolar disorder, or substance use disorders
- High baseline anxiety symptoms or frequent panic attacks
- Biological factors involving neurotransmitter dysregulation in the CNS
- Chronic stress or trauma leading to Post-Traumatic Stress Disorder (PTSD)
For many, this struggle is not due to lack of willpower but rather neurochemical, environmental, and genetic complexity that standard treatments alone can’t always resolve.
Pharmacologic Treatment Options Beyond SSRIs
When traditional SSRIs such as sertraline, paroxetine, or escitalopram fail, clinicians may consider alternative or augmentation strategies. Pharmacologic treatment in resistant cases is about precision—balancing efficacy, tolerability, and patient safety.
Second-line and adjunctive medications may include:
- SNRIs such as venlafaxine or duloxetine for persistent GAD and panic disorder
- Buspirone, a non-benzodiazepine anxiolytic, effective for mild-to-moderate anxiety
- Pregabalin or gabapentin, anticonvulsants shown to reduce GAD symptoms in several randomized controlled trials (RCTs) (Biol Psychiatry)
- Hydroxyzine, an antihistamine sometimes used short-term for acute anxiety
- Atypical antipsychotics such as quetiapine or olanzapine, occasionally used in augmentation for refractory cases (Psychopharmacol, Clin Neurosci)
- Benzodiazepines, while effective, are typically reserved for short-term use due to dependence and discontinuation concerns (Rickels K, Depress Anxiety, 2008)
Emerging treatments, like ketamine and transcranial magnetic stimulation (TMS)—approved by the FDA for treatment-resistant depression—are being explored for anxiety with promising early results.
The Role of Psychotherapy and Behavioral Interventions
While medication helps manage physiological symptoms, psychotherapy remains the cornerstone of effective treatment for anxiety. When standard CBT doesn’t yield results, newer or combined behavioral therapy models may help overcome resistance.
Advanced interventions include:
- Exposure therapy, particularly for phobias, OCD, and panic disorder
- Mindfulness-based CBT, which integrates mindfulness and acceptance to reduce avoidance behaviors
- Functional and emotion-focused therapy, aimed at reworking family dynamics and interpersonal patterns contributing to anxiety
- Transdiagnostic CBT, designed to address overlapping symptoms across mood disorders and psychiatric disorders
Evidence from meta-analyses (Pollack MH; Stein MB; J Clin Psychiatry) shows that combining psychotherapy and pharmacotherapy significantly improves outcomes for treatment-refractory anxiety compared to either alone.
Biological and Neuromodulation Approaches
For those who don’t respond to traditional interventions, neuromodulation may represent a new frontier in the treatment of anxiety.
Options under clinical investigation or use include:
- TMS (Transcranial Magnetic Stimulation) – non-invasive stimulation of specific brain regions linked to GAD and PTSD
- Vagus Nerve Stimulation (VNS) – targets autonomic regulation and emotional control pathways
- Ketamine infusions – fast-acting NMDA receptor antagonists that show potential for resistant anxiety and depression
While more double-blind, placebo-controlled trials are needed, early findings suggest neuromodulation could be life-changing for individuals with severe, persistent anxiety symptoms unresponsive to medication.
Emerging Evidence and Future Directions
Recent clinical trials and meta-analyses published in journals such as J Clin Psychiatry, Biol Psychiatry, and Am J Psychiatry continue to refine how we understand treatment-resistant anxiety. Researchers are exploring:
- Novel pharmacologic agents targeting GABAergic and glutamatergic systems
- Extended-release formulations for improved tolerability and compliance
- Precision psychopharmacology based on genetic and biological markers
- Combined use of mindfulness, CBT, and pharmacologic treatment to enhance treatment outcomes
The next decade of anxiety care may lean heavily toward integrated, data-driven approaches that merge evidence-based psychiatry, technology, and holistic mental health models to achieve deeper, faster remission.
When Anxiety Becomes a Shared Battle
Behind every resistant case of anxiety is a person—and often, their loved ones—fighting to reclaim stability. It’s critical that primary care and mental health providers coordinate care to ensure every angle is addressed: biological, psychological, and social. For some, recovery may involve revisiting previous interventions with new insight or combining approaches once thought incompatible.
Key takeaways:
- Reassess diagnosis and comorbidities using DSM-5 criteria
- Ensure adequate trial length and dosage for SSRIs/SNRIs before labeling resistance
- Explore augmentation with atypical antipsychotics, anticonvulsants, or buspirone
- Integrate CBT, exposure therapy, and mindfulness into ongoing care
- Prioritize continuity between clinicians, psychiatrists, and therapists
Moving Forward with Safe & Sound Treatment
At Safe & Sound Treatment in Costa Mesa, CA, our clinicians combine psychotherapy, CBT, and personalized pharmacologic treatment to help clients facing complex or treatment-resistant anxiety disorders. Serving the Orange County area, we specialize in evidence-based care—whether you’re navigating panic attacks, social anxiety, or GAD that hasn’t improved with standard methods.
Our compassionate team creates individualized treatment plans that integrate traditional psychiatry with holistic, research-informed approaches to promote lasting relief and mental balance.
Call (949) 449-2795 today to learn more about how Safe & Sound Treatment can help you find the next step on your recovery journey.